October 13, 2003
Life on Earth is
Definitely not for the Faint-Hearted
(So how is it that we can stand up to gravity?)
By Dr. Howard Glicksman
Remember last month? Clint Eastwood and his character, The Man With No Name
from the movie The Good, The Bad and the Ugly, demonstrated to us the importance
of fluid balance in the body.Ā If you missed that column or you’d like
to review it first you can do so here. This month The Man With No Name has more to teach
us as we read in Life on Earth is not for the Faint-Hearted (So how is it that
we can stand up to gravity?).Ā
Let’s return to our hero, played by Clint Eastwood, in the movie, The
Good, The Bad and The Ugly.Ā He is weaving and staggering under the physical
strain of heat prostration and dehydration as he is forced to trudge through
the desert.Ā Just when he is about to be put out of his misery by a bullet to
the head, a black stagecoach appears on the horizon.Ā Several scenes later,
after our hero has learned the secret whereabouts of buried treasure, he conveniently
faints, thereby preventing his torturer from further interrogating him.
Is this another example of Hollywood pointing a finger of affirmation toward
the intelligent design of life?Ā Well, yes and no.Ā Yes; if one is inclined
to try to understand how it is that the body is capable of standing up against
gravity in order to be able to faint when things inside just don’t work
right.Ā And, No; if one is not interested in how the body actually works
and is happy to accept and trust the conclusions made by others.Ā Are you ready
to test what you believe to be true about macroevolution?Ā Then read on my friend.
Quite simply, one faints when one’s blood pressure drops so low that not
enough blood is going to the brain.Ā There are many mechanisms in the body that
are involved in maintaining an adequate blood pressure and blood flow to the
tissues.Ā As you may have guessed by now, the body’s ability to stand up
against gravity is more complicated than just considering its bones and muscles.Ā
One must have enough blood coursing through the vital organs of the body in
order to provide them with water, nutrients and oxygen to allow them to function
properly.Ā The blood pressure, which is a measure of the force that the blood
exerts against the arterial wall, plays a significant role in our survival.Ā
How do we know this to be true?Ā In one word: SHOCK.
No, not the shock that you see portrayed in movies when someone faints or is
in a catatonic state due to a sudden emotional or psychological insult.Ā I mean
circulatory shock or collapse, which is a medical emergency in which the body
is not able to adequately supply the tissues with enough nutrients and oxygen
to meet their metabolic needs.Ā There are many signs that we see when someone
goes into circulatory shock, but one of the commonest is a severe drop in blood
pressure.Ā And why is it such an emergency?Ā In two words: irreversible damage,
leading to certain death.
There are basically three fundamental components of the circulatory system:
the circulating blood volume, the pumping action of the heart, and the vascular
system which consists of the arteries, veins and the microcirculation which
involves the arterioles, the capillaries and the venules.Ā The arterioles and
venules have small muscles around them that contract and relax to different
degrees in order to control the flow of blood in the tissues.Ā More to the point,
if the arterioles did not provide some resistance to blood flow, then the blood
pumped by the heart would freely enter the microcirculation and overwhelm the
capillaries while at the same time severely diminishing the effective blood
volume and lowering the blood pressure.ĀĀĀ
A breakdown in function of any of these three fundamental components can result
in circulatory shock and death.Ā For example, the blood volume can be seriously
compromised if someone starts bleeding from an internal injury, such as from
a car accident or from recurrent vomiting and diarrhea without adequate rehydration.Ā
The pumping action of the heart may be significantly reduced or even totally
ineffective if someone has a heart attack, which causes damage and weakens the
heart muscle, and then suffers a cardiac arrest.Ā Lastly, there are many conditions,
particularly septic shock from severe infection, that can cause the microcirculation
to malfunction by dilating and allowing blood to pool within tissues and thereby
be lost to the circulation which results in irreversible shock and death.Ā Ā
The body has many different ways of monitoring and controlling all three of
these vital components of the circulatory system so that we may stay alive.Ā
It does this moment to moment and without us having to worry about it. ĀWhen
was the last time you checked if you had enough blood in your circulation, if
your heart was pumping well enough, or your peripheral vascular resistance was
up to snuff?
Having too low of a blood pressure can be life-threatening as we’ve just
stated above.Ā But what about high blood pressure?Ā I’m sure that many
of you are familiar with it being a risk factor for stroke, heart disease and
kidney failure.Ā By investigating the various causes and thereby developing
treatments for hypertension, modern medicine has stumbled upon one of the most
important of these blood pressure/blood flow monitoring systems which I’d
like to briefly tell you about this month.Ā It’s called the renin-angiotensin
system or RAS as it’s referred to in the business.Ā Now don’t be frightened
by all of these fancy scientific names.Ā By the time you finish this column,
you’ll have a pretty good understanding of how all of this works to keep
you alive and I suspect that you’ll be scratching your head as to how it
could have all developed simply by the random forces of nature.ĀĀĀĀ Ā
Say hello to the hormone called, angiotensin II, the strongest known
arteriolar muscle tightener known to the body.Ā It’s constricting action
is about five times stronger than adrenaline, the stuff you’ll often see
injected into dying patients when you’re watching a medical scene in the
movies or on television.Ā Angiotensin II also has the ability to stimulate
the adrenal gland to produce and secrete another hormone that will make the
kidney hold onto more water and sodium.Ā So you can see that when angiotensin
II Āis on the job, it is directly affecting two of the three fundamental
components that maintain the body’s circulation.Ā Its vasoconstrictor activity
affects the peripheral downstream resistance applied by arterioles to increase
the blood pressure, and its ability to positively affect sodium and water retention
directly affects the blood volume.Ā Let’s look at where angiotensin
II comes from and how the body controls its production.ĀĀ
 In
order for angiotensin II to be produced, the body requires the services
of the liver, the kidneys, the lungs and the circulation.Ā The liver produces
an inactive protein called angiotensinogen, which floats around in the
bloodstream doing absolutely nothing.Ā But don’t give up yet, the body’s
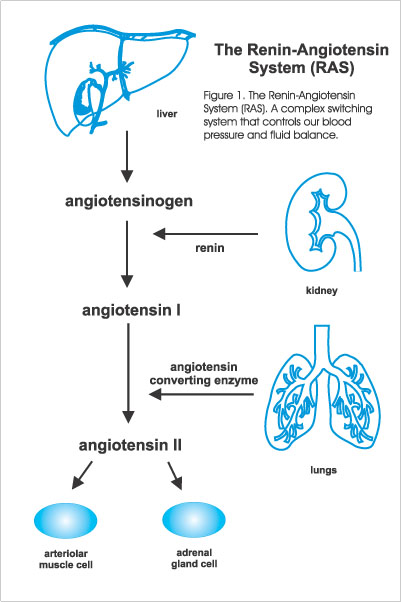
got it all figured out already (see Figure 1).
In
order for angiotensin II to be produced, the body requires the services
of the liver, the kidneys, the lungs and the circulation.Ā The liver produces
an inactive protein called angiotensinogen, which floats around in the
bloodstream doing absolutely nothing.Ā But don’t give up yet, the body’s
got it all figured out already (see Figure 1).
The kidney contains specialized cells which are located near where it starts
the filtering process on the way to forming urine, that are sensitive to the
pressure of blood flow.Ā These specialized cells secrete a hormone called renin
at a rate that is inversely proportional to the blood flow that they detect.Ā
So if the blood flow is very low they will secrete more renin and if
it is adequate they will reduce the flow to maintenance levels and if the flow
is above what is necessary, they will reduce the production and secretion of
renin.Ā OK so far?Ā Then let’s continue.Ā ĀĀ
Now comes the interesting part.Ā Remember that apparently useless protein called
angiotensinogen that is produced in the liver?Ā Well, when it comes in
contact with renin it is chemically converted into another protein called
angiotensin I which is also inactive in the body.Ā Close but no cigar!Ā
How do we eventually get the vasoactive hormone called angiotensin II
?Ā
The cells that line the blood vessels in the lungs secrete a protein called
angiotensin converting enzyme, which when it acts on angiotensin
I that is floating in the circulation, chemically converts it to angiotensin
II. ĀAnd voila, we now have the most powerful arteriolar muscle tightener
in the body.Ā A chemical messenger that is vital for maintaining the blood pressure
and thereby allowing the circulation to meet the body’s metabolic needs.Ā
But the story doesn’t end there.Ā For the muscles surrounding the arterioles
and the adrenal cells cannot be affected by the angiotensin II molecule
unless their cell membranes contain angiotensin II receptors where the
hormone locks on and causes the desired effect.Ā The system works much like
what you may have seen in the movie True Lies where Arnold Schwarzenegger’s
character has his right handprint and right retina analyzed to verify his identity.Ā
The arteriolar muscle cell and the adrenal cell won’t play with strangers!Ā
But remember, that in order for the body to be able to adequately control each
vital function, once it turns on a switch it needs to be able to turn it off
as well.Ā Otherwise, the reactions set in motion by a given amount of angiotensin
II could result in marked elevations in blood pressure and sodium retention.Ā
The combined actions of Ārenin andĀĀ angiotensinĀ convertingĀ enzyme
onĀ angiotensinogen and angiotensin I, respectively as they travel
in the circulation results in the turning on of the switch.Ā What turns it off?Ā
In fact, the effects of angiotensin II are short-lived because there
are many other proteins contained in the tissues and red blood cells that are
able to chemically break it down so that a given amount in the circulation is
only effective for about ten minutes.Ā These proteins, that are enzymes, are
collectively known as angiotensinases.
Now when you consider all of the components that are necessary for the RAS
to work, it seems to me that the NeoDarwinian mechanics of macroevolution just
don’t stand up to scrutiny.Ā Let’s look at what macroevolutionists
must scientifically be able to prove here before anyone should even consider
macroevolution as a truth of science.
There are six major factors at play here:
- The liver cell that produces what at first glance would seem to be a biologically
useless protein called angiotensinogen.Ā Remember, without renin,
the production of angiotensinogen by the liver would appear
to be against the law of survival of the fittest, because it would
be wasting nutrients and energy on producing useless biological junk proteins.Ā
Efficiency is what is necessary to win the battle.
- There’s the specialized kidney cell that just happens to be in the
right place to be able to detect the flow of blood coming into the kidney
and at the same time be able to produce and secrete renin, which ultimately
has a direct effect on blood pressure and blood volume.Ā The cell is able
to vary the secretion of renin by an inverse relationship to the changes
in blood flow that it detects ĀThis is absolutely necessary for body survival.
- Renin’s main action is to convert angiotensinogen, that
is floating around in the circulation, into another inactive protein
called angiotensin I .Ā At this point all three of the proteins involved
are incapable of accomplishing anything of importance for bodily function.
- The cells lining the circulation of the lungs produce and secrete a protein
called angiotensin converting enzyme which acts on angiotensin I
as it floats by in the circulation so that it morphs into the strongly vasoactive
protein known as angiotensin II. ĀThis hormone ultimately affects blood
pressure and fluid balance allowing the circulation to adequately supply the
tissues with nutrients, oxygen and water.
- The angiotensin II molecule can only exert an effect on the arteriolar
muscle cell and the adrenal gland cell by interlocking with an angiotensin
II receptor site on the cell membrane.Ā Without this receptor, angiotensin
II itself, would be biologically useless to the body.
- In order that this system may have a biologically necessary moment to moment
sensitivity and responsiveness which will allow for survival, the body contains
enzymes that are capable of breaking down angiotensin II in an orderly
fashion so that it only has a short-lived effect in the body.Ā
ĀAs a scientist, I believe that those who promote and teach macroevolution
as a well-proven theory must explain the development of each and every one of
the proteins involved in this system.Ā But it’s not sufficient to only
explain how they each came into being.Ā One must also explain how this system
could have been functional absent any combination of the above vital components;
for that is how macroevolutionary mechanics works, one step at a time over many
generations.Ā For if the body were not able to properly control its blood pressure
and blood volume, then there’s no use in discussing further generations
because the body would not be able to survive.Ā
Based on the current understanding of human physiology and the pathological
processes that undermine bodily function, we have ample clinical evidence of
what happens when one or more of these vital components for our survival are
compromised, never mind being totally absent.Ā One need only theorize on how
the system one step beforehand worked and then continue the process backwards
in order to confirm macroevolution’s thesis.Ā
Any discrepancy between known data and a given theory is sufficient to undermine
that theory’s validity no matter what has supported it in the past.Ā It
must either be abandoned or amended to fit the data.Ā This is much akin to how
Copernicus improved upon Ptolemy and Kepler improved upon Copernicus when considering
astronomical data.Ā Or how Newton improved upon Aristotle and Einstein improved
upon Newton regarding physics.Ā ID may be an alternate theory to macroevolution.
But one has to let go of the currently held theory of macroevolution before
one can even begin to consider any other alternative.
Now here are some examples of questions that I think need to be answered before
anyone should be embracing macroevolution as a well-proven theory.
- Which came into existence first, angiotensin II, or the angiotensin
II receptor? If the hormone existed before the receptor, how did it exert
its effect?Ā If the receptor existed before the hormone, then what useful
purpose did it serve?
- If the RAS could only develop one step at a time by genetic mutation then
that would mean that only one protein at a time could come into existence.Ā
Please explain how the necessary proteins, angiotensinogen, renin, and
angiotensin converting enzyme came into existence, in what order and what
purpose did they serve to the body before they were present as an integrated
unit?
- Which came into existence first, the angiotensin II molecule or
the angiotensinase enzyme which breaks it down in the circulation?Ā
If the molecule existed first without the enzyme, then how did
the body control the effects of the molecule on blood pressure and blood volume?Ā
If the enzyme existed before the molecule, then what useful purpose did it
serve for the body?
Maybe you can come up with some answers or further questions on this subject.Ā
Let me know, I’d like to hear from you.Ā Why not post me a message at the
ARN Discussion Forum?Ā
I can’t promise to respond to every message but I will attempt to read
them all.
Critics who have written to me so far have helped make me organize my thoughts
better on this issue and I thank them for their efforts.Ā
Taking into account my knowledge of how the human body works, it is my humble
opinion that these questions are indeed unanswerable.Ā In addition, it is my
opinion that it is more difficult to believe that these complex, interdependent
systems could have developed by random chance than it is to believe that they
have come about by intelligent design.Ā One critic commented that “IDists…have
a vested interest in proving ICness”.Ā Having been on both sides of the
fence at one time or another, I think that the same could be sincerely said
of macroevolutionists regarding their theory as well. ĀFinally, what will constitute
proof to any one individual of the impossibility of a given event other than
the intellect and beliefs of that one individual?Ā Intelligence is often in
the mind of the beholder!Ā And by the way, so is the lack of intelligence!!
The next two columns are going to touch on a subject and substance that is
very important to paleontologists.Ā Does the fact that similar species having
similar bone structure prove the theory of macroevolution?Ā ĀNot quite when
you consider how those bones were actually formed by those bodies.Ā One might
similarly ask if the fact that bicycles and motorcycles being very similar in
structure proves that they came into existence by the random forces of nature?Ā
I think you’ll find the study a fascinating one that should leave you with
questions you can ask your science educators to answer in order to verify the
validity of macroevolution.
Dr. G.
Howard Glicksman M.D. graduated from the University of Toronto
in 1978.Ā He practiced primary care medicine for almost 25 yrs in Oakville,
Ontario and Spring Hill, Florida.Ā He recently left his private practice and
has started to practice palliative medicine for a Hospice organization in his
community.Ā He has a special interest in how the ethos of our culture has been
influenced by modern science’s understanding and promotion of what it means
to be a human being.
Copyright 2003 Dr. Howard Glicksman. All rights reserved. International
copyright secured.
File Date: 10.13.03